Technology
Multimodal
hemoadsorption
Efferon hemoadsorption technology is designed to help restore immune balance by directly eliminating endotoxin and excessive inflammatory mediators from the bloodstream, addressing dysregulated inflammation at its source.
Inflammation as a core driver of critical illness
Inflammation is a protective host response to infection or tissue injury. In sepsis, this response becomes dysregulated and can contribute to endothelial injury, circulatory dysfunction, and multi-organ failure. Septic shock represents the most severe end of this spectrum.
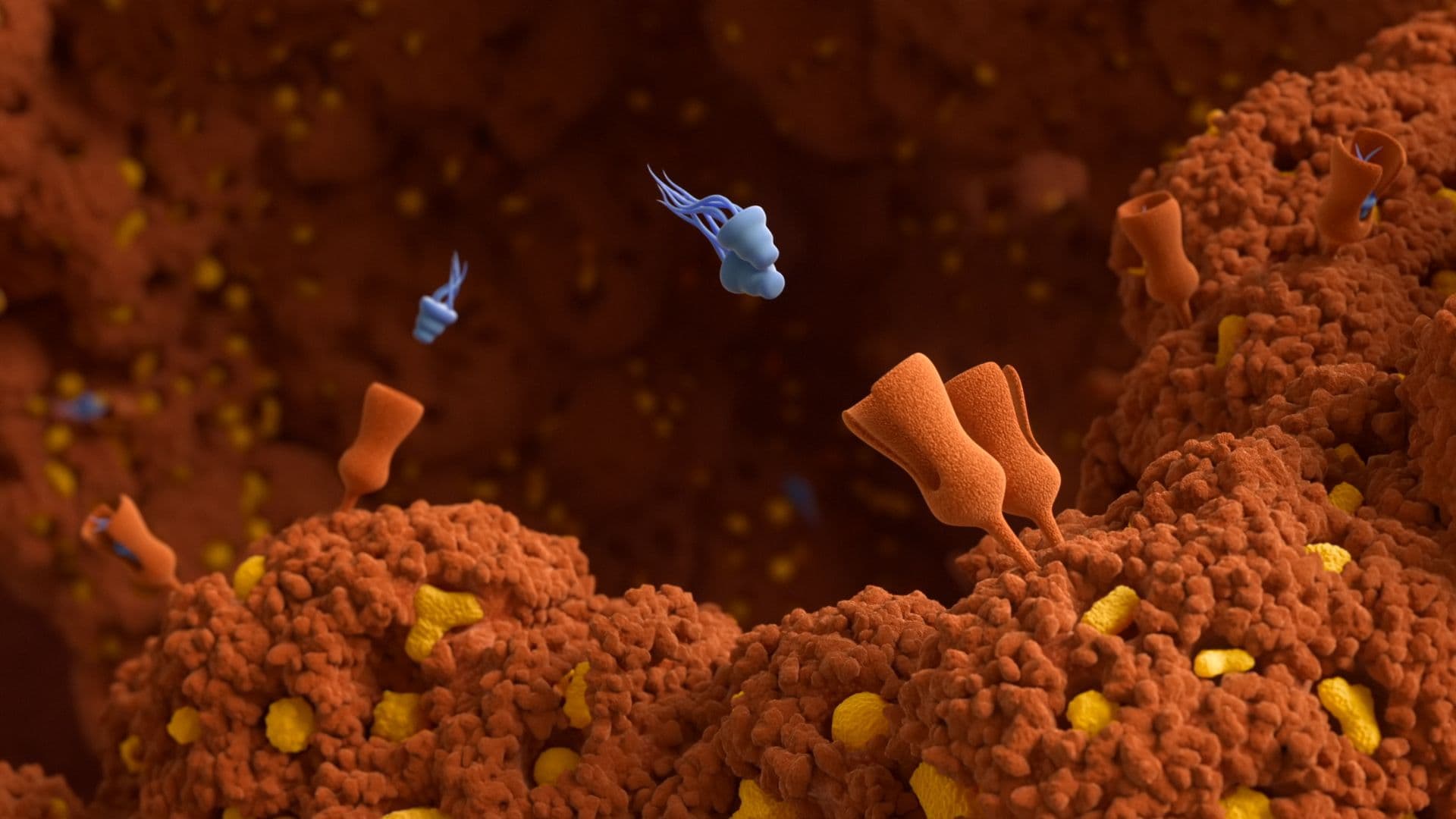
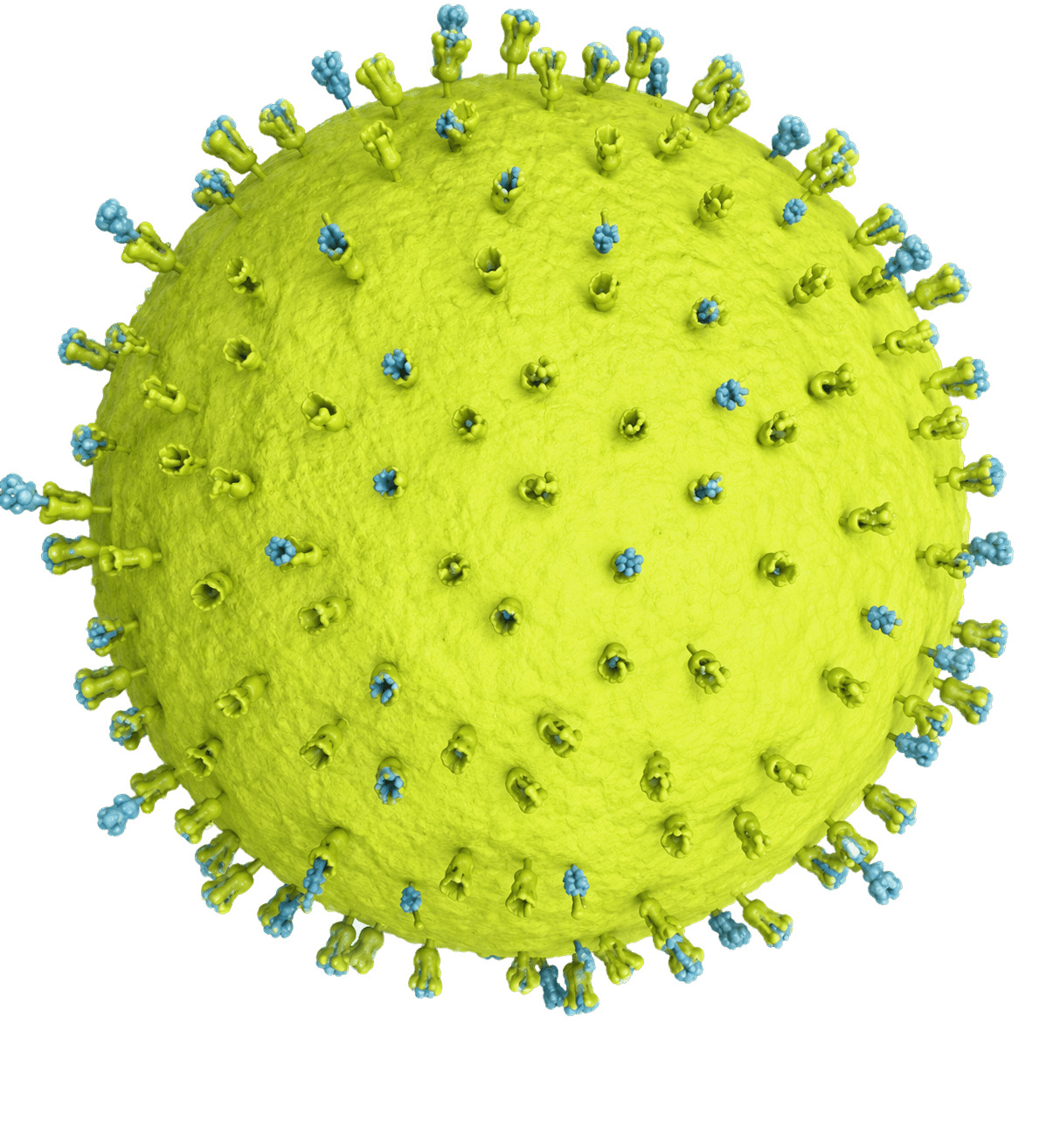
Among the key drivers of this dysregulated response is endotoxin (lipopolysaccharide, LPS) (Fig 1), a structural component of the outer membrane of Gram-negative bacteria. Endotoxin may enter the circulation through multiple pathways, including bacterial infections (such as pneumonia, intra-abdominal, urinary tract, and bloodstream infections), and, in the context of major surgery or traumatic insult, via increased intestinal permeability with subsequent translocation from the gut lumen into the bloodstream. In the latter case, disruption of the gut barrier — associated with critical illness, ischemia-reperfusion, or infection — may allow translocation of endotoxin into the bloodstream.
Once in circulation, endotoxin can activate innate immune pathways, including Toll-like receptor 4 (TLR4) signaling, and contribute to the release of inflammatory mediators such as cytokines TNF-α and IL-6 (Fig 2). When excessive, this response may lead to vasodilation, increased vascular permeability, hemodynamic instability, impaired tissue perfusion, and progressive organ dysfunction.
The unmet need in extracorporeal blood purification
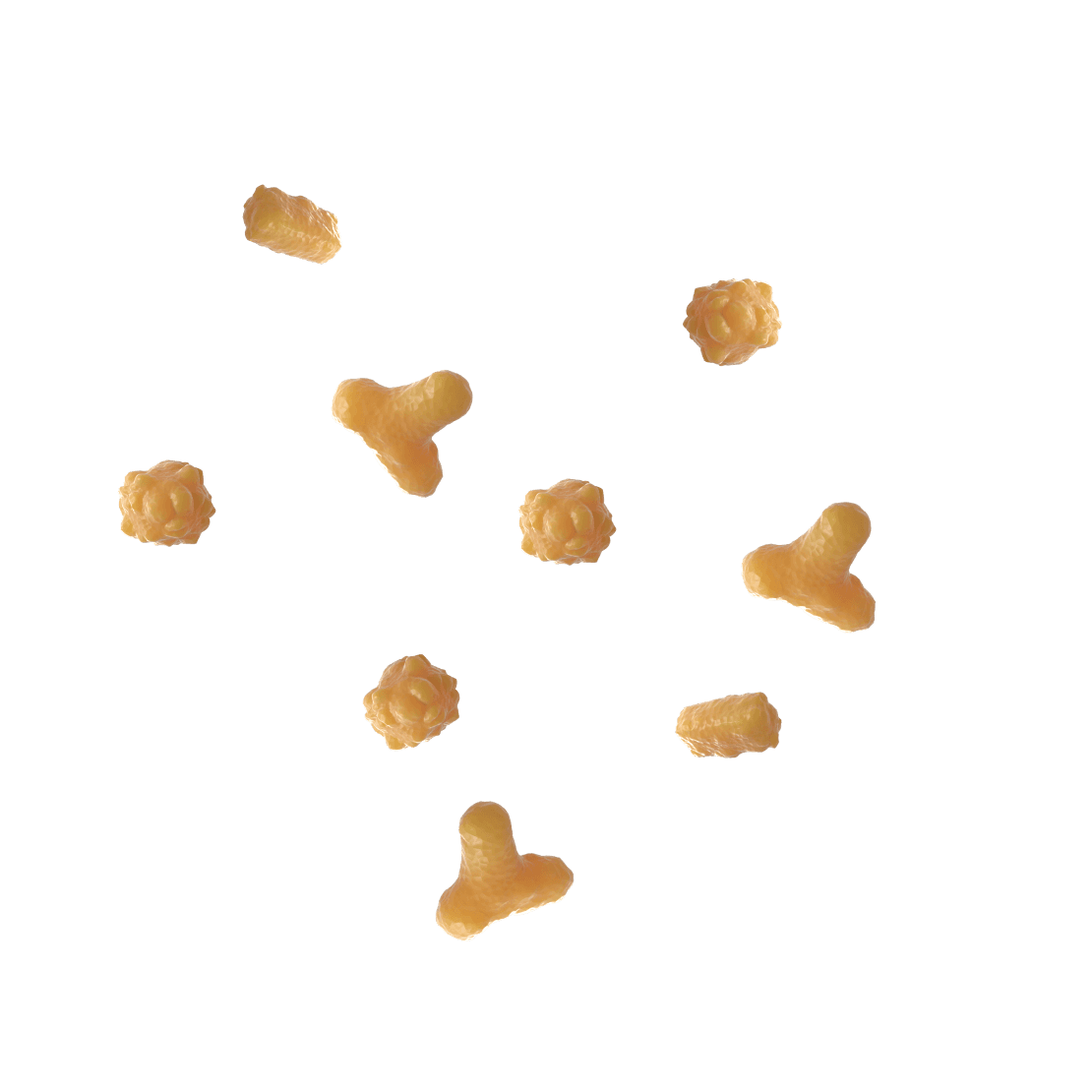
Potential therapeutic targets for sepsis and multiple organ failure are bacterial endotoxins (lipopolysaccharides, LPS), cell debris (DAMP), and an excess of inflammatory regulators (cytokines).
Specific pharmacotherapy aimed at these targets is ineffective or has severe side effects. Therefore, methods of direct (extracorporeal) removal of these compounds from the body are taking the leading role in the complex therapy of these conditions. But existing technologies only affect one part of the process instead of a comprehensive impact.
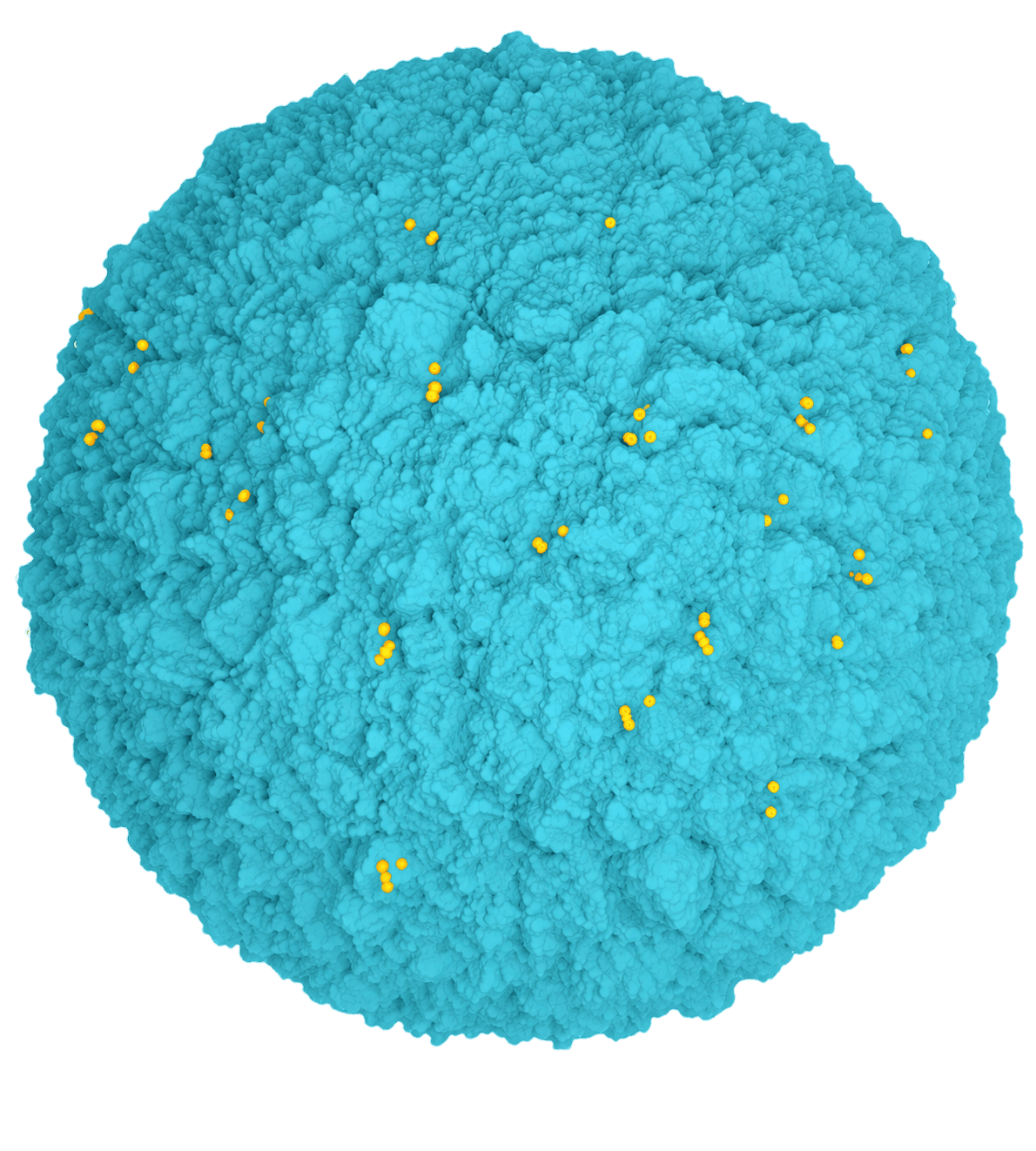
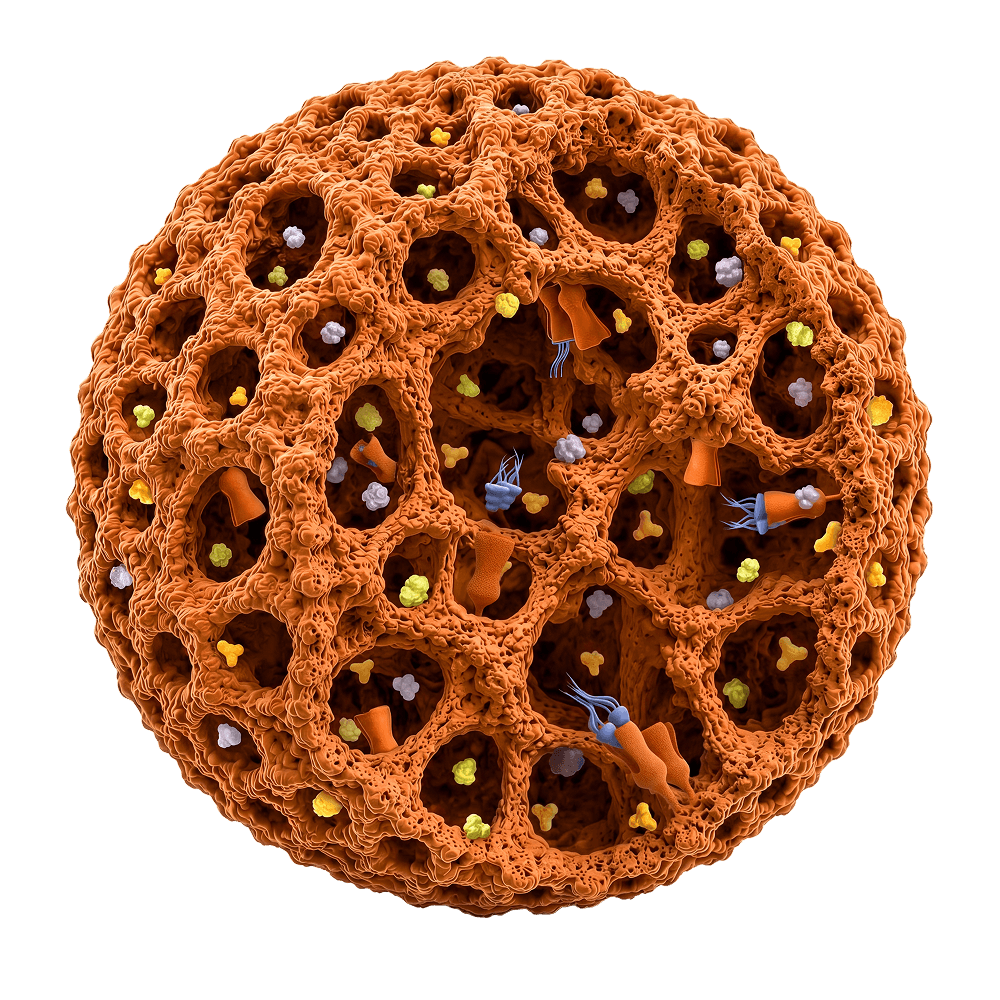
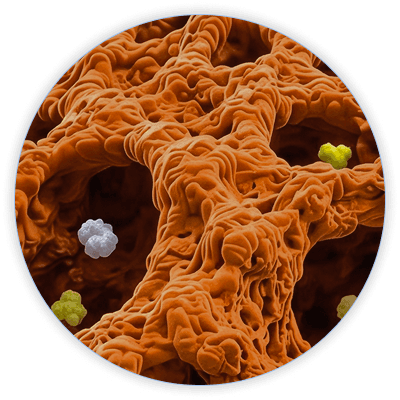
Porous non-selective adsorbents (Fig 3) are applied to remove excessive cytokines and cell debris (DAMP). The molecular structure of LPS prevents its binding by such adsorbents. To remove LPS, surface-modified materials with immobilized selective ligands are used. However, adsorbents of this structure do not possess the mesoporous structure required to absorb the excess of cytokines.
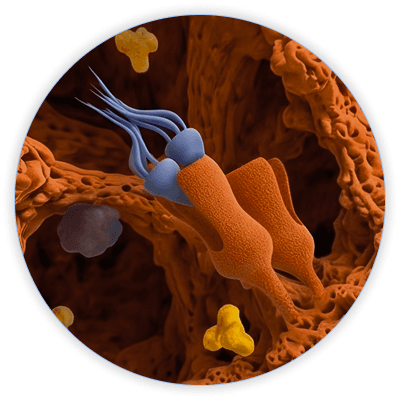
LPS-selective adsorbents (Fig 4) don't have pores of the required diameter and morphology for effective removal of excess cytokines and other exo- and endogenous toxins. The porous structure of non-selective adsorbents does not yield efficient removal of associates and micelles of lipopolysaccharides from the whole blood.
The dysregulated immune response is a core driver of chronic critical illness. The underlying mechanism, known as the persistent inflammation, immunosuppression, and catabolism syndrome, involves a prolonged state of both inflammation and immune suppression. This condition increases the risk of secondary infections and contributes to significant muscle wasting, leading to poor long-term outcomes. This vicious cycle is associated with worse long-term outcomes and increased mortality risk.
Next-Generation Multimodal Hemoadsorption
To address this unmet need, Efferon developed a multimodal hemoadsorption approach. Multimodal hemoadsorption is an extracorporeal blood purification approach designed to act directly within the bloodstream, where dysregulated inflammation becomes clinically significant. Efferon LPS adsorbent is the first multimodal adsorbent that simultaneously removes both the cause of excess inflammation — LPS — and excess inflammatory molecules from the bloodstream.
As blood passes through the device, it encounters engineered polymer beads (Fig 5) with a multimodal design:
- On the surface, a selective ligand is designed to bind endotoxin (LPS) through high-affinity interactions
- Within the porous structure, the beads enable adsorption of circulating inflammatory mediators, including cytokines
1st component: Hypercrosslinked polystyrene matrix
The matrix (Fig 6) consists of a synthetic polymer with a rigid, three-dimensional porous structure. First developed and characterized by Davankov and Tsyurupa, these materials stand out for their exceptionally high porosity, reaching a specific surface area of 700–900 m²/g, far beyond that of most organic polymers. They also exhibit low thrombogenicity. Their internal structure includes large closed pores with diameters of up to 100 nm, connected by a network of much narrower channels that permeate the matrix.
The adsorption of cytokines in the pores proceeds according to a nonspecific mechanism and is a reversible equilibrium process. As a result, the degree of removal turns out to be higher for the protein initially present in a higher concentration. Thus, in the course of hemoperfusion through such adsorbents, cytokine clearance decreases over time. Such a mechanism is appropriate to reduce the peak concentrations of these important inflammatory mediators while maintaining levels above zero. This approach does not lead to the complete depletion of cytokines, but rather modulates their concentrations, guiding the immune system back toward a state of homeostasis.
2nd component: Synthetic ligand to the lipid
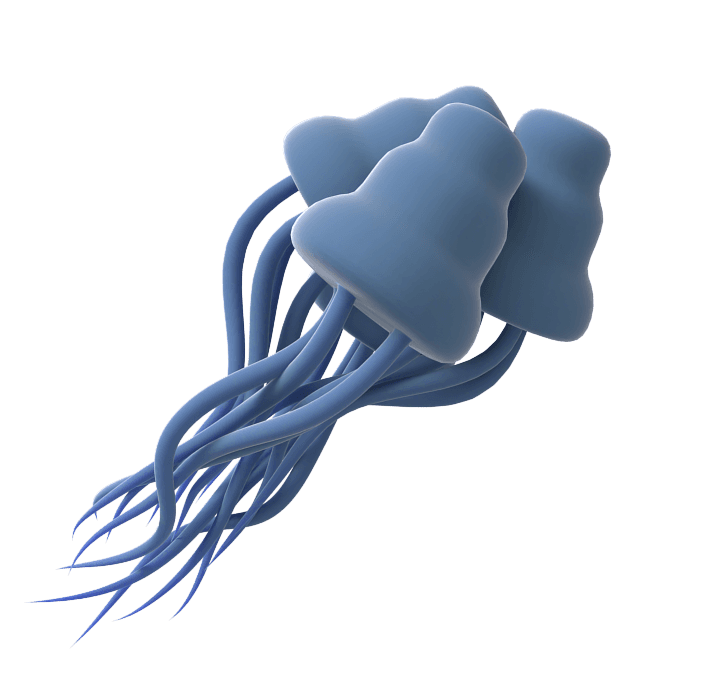
The sorbent on the surface features a specially designed "ligand" (Fig 7) to bind LPS through high-affinity interactions.
In the bloodstream, individual LPS molecules are small, but they clump together with blood proteins to form enormous complexes. This makes them difficult to filter out using simple size-based methods, as conventional adsorber can't effectively catch both the small individual molecules and the huge clumps.
Efferon approach solves this problem by using the ligand's strong, irreversible bond instead of relying on filtration. Bench-top experiments show the difference clearly: a standard filter material left elevated levels of LPS in the blood. But when the same material was enhanced with specific ligands, it captured the LPS so effectively that its concentration dropped to well below clinically significant levels.
References
- Bessonov I.V., Morozov A.S., Kopitsyna M.N. A polymeric sorbent, preparation and use thereof, patent No WO2018217137, 2018.
- Magomedov M.A., Kim T.G., Masolitin S.V., Yaralian A.V., Kalinin E.Yu., Pisarev V.M. Use of sorbent based on hypercrosslinked styrene-divinylbenzene copolymer with immobilized LPS-selective ligand in hemoperfusion for treatment of patients with septic shock. General Reanimatology. 2020;16(6):31-53.
- Davankov V.A., Rogozhin S.V., Tsjurupa M.P. Macronet polystyrene structures for ionites and method of producing same, patent No US3729457A, 1973.
- Davankov V.A., Tsyurupa M.P. Structure and properties of hypercrosslinked polystyrene — the first representative of a new class of polymer networks. Reactive Polymers. 1990;13(1-2):27-42.
- Honore P.M. et al. Cytokine removal in human septic shock: where are we and where are we going? Annals of Intensive Care. 2019;9(1):56.
- David S.A. Towards a rational development of anti-endotoxin agents: novel approaches to sequestration of bacterial endotoxins with small molecules. Journal of Molecular Recognition. 2001;14(6):370-387.
- Caroff M., Karibian D. Structure of bacterial lipopolysaccharides. Carbohydrate Research. 2003;338(23):2431-2447.
- Morozov A.S. et al. A selective sorbent for removing bacterial endotoxins from blood. Russian Journal of Physical Chemistry A. 2016;90(12):2465-2470.
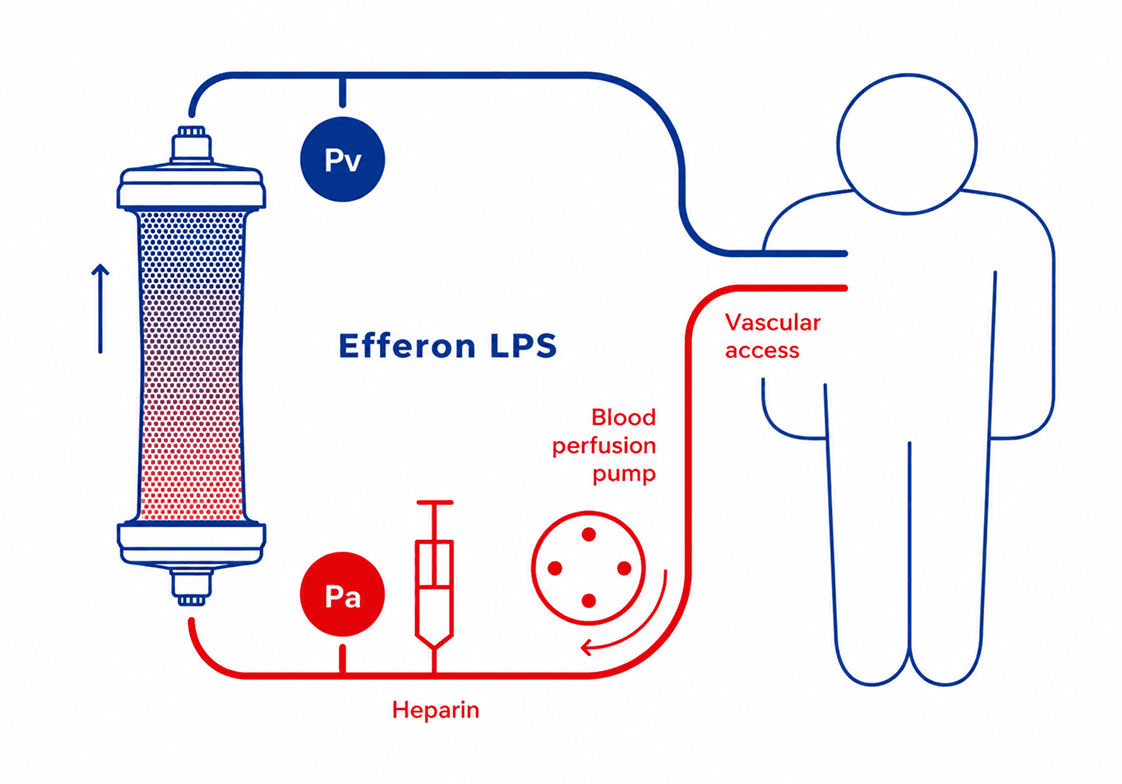
How multimodal hemoadsorption device works
The sorbent is loaded into a next-generation extracorporeal blood adsorber, a non-pyrogenic, gamma-sterilized, single-use medical device designed for hemoadsorption. It provides selective adsorption of lipopolysaccharides and non-selective adsorption of cytokines, myoglobin, cellular debris, and endogenous and exogenous toxic substances.
Designed for seamless integration into contemporary extracorporeal support platforms used in intensive care units, the device is compatible with standard hemoperfusion circuits and can be readily incorporated into renal replacement therapy (RRT), extracorporeal membrane oxygenation (ECMO), and cardiopulmonary bypass (CPB) systems. Its standardized connectors, low flow resistance, and straightforward integration enable flexible use across a wide range of critical care applications.
By reducing circulating levels of endotoxin and inflammatory mediators, the device may help mitigate excessive systemic inflammation. Early incorporation into extracorporeal blood purification strategies may support hemodynamic stabilization and preservation of organ function in septic patients.
Clinical Experience and Reported Outcomes
Multimodal hemoadsorption has been evaluated in randomized and controlled clinical studies in critically ill patients. Clinical data demonstrate consistent effects on key pathophysiological targets of sepsis.
Across studies, treatment was associated with:
- Faster resolution of septic shock
- Early hemodynamic improvement
- Reduced vasopressor requirements during acute phase
- Rapid decline in inflammatory markers (IL-6, CRP, PCT within 24–72 hours)
- Rapid recovery of organ function reflected by improvement in SOFA score
In selected patient populations, differences in mortality have also been reported in patients with septic shock; outcomes may vary depending on patient characteristics, timing of intervention, and study design.